Follow the Data Podcast: Global Health Check-Up with Dr. Kelly Henning
Tobacco is a deadly killer, claiming over seven million lives every year, with most of the deaths occurring in low- and middle-income countries. Mike Bloomberg has been committed to tobacco control since first entering office as New York City Mayor, and Bloomberg Philanthropies has invested one billion dollars to help implement tobacco control measures.
Dr. Kelly Henning leads Bloomberg Philanthropies’ Public Health programs. She’s been on the road, visiting countries across the world, as part of a “global health check-up.” She spoke to the foundation’s operations lead, Allison Jaffin, about the progress countries are making, sharing lessons learned and stories from the road.
You can listen to the podcast and past episodes in the following ways:
- Check us out on Spotify
- Download the episode from iTunes and be sure to subscribe
- Follow the Data is available on Stitcher – be sure to rate and review each episode
- Stream the podcast on Simplecast
- Listen to the episode and follow us on SoundCloud
FULL TRANSCRIPT
KATHERINE OLIVER: Welcome to Follow the Data, I’m your host, Katherine Oliver.
When tackling some of the toughest public health challenges like tobacco control and road safety – how well are countries around the world actually doing?
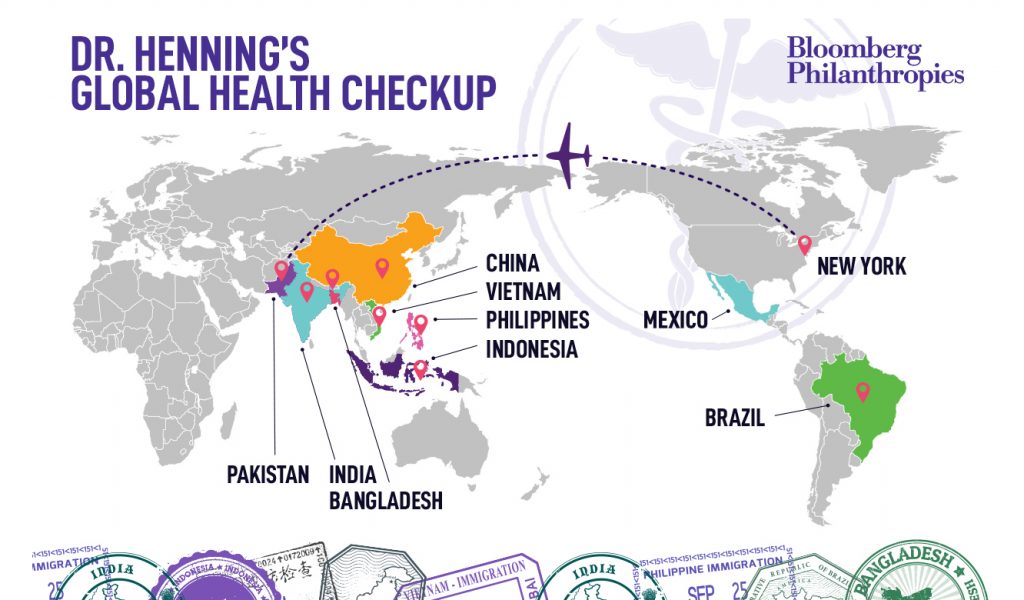
Throughout the past year, Bloomberg Philanthropies public health program lead Dr. Kelly Henning visited Brazil, Vietnam, China, Indonesia, the Philippines, Pakistan, Bangladesh, and India to see firsthand the successes and challenges our partners face in tackling injuries and non-communicable diseases (also known as N-C-Ds) in their communities.
Back from her travels, Dr. Henning sits down with Bloomberg Philanthropies’ operations lead Allison Jaffin to share more about what she’s seen from her “Global Health Check Up” tour and what keeps her optimistic about the future of public health.
ALLISON JAFFIN: Hi, Kelly. Thank you for joining us today. I know we get to talk nearly every day at the office when you’re not traveling, but I’m excited that we get to share with our listeners today, some of the incredible life-saving work you’re witnessing, and we’re supporting around the world, so let me be the first to say, welcome back from your world tour, and I thought maybe we could start by discussing the reasons why you took this journey.
DR. KELLY HENNING: Thanks, Alli. It’s so exciting to be able to talk about this tour. It was really a new approach for me personally, and I was really excited to get out there and go country by country, and talk to the various folks on the ground who are really in the trenches doing this work each and every day. The idea here was to really understand the work from the perspective of the people on the ground, so we often, as funders, hear things in written reports, but we don’t always hear the voices of those people out there really doing the work on the ground, so it was a fantastic opportunity. I was so glad to have a chance to do that, and I really learned a lot.
JAFFIN: I think we’ve referred to this internally as a global health checkup, aside from just getting firsthand accounts, can you walk us through what you’re doing or seeing on the ground?
DR. HENNING: Absolutely, so what we do is, we do a lot of preparation work before the tour begins, so we reach out to folks that are working in a particular country, and we ask for advice about who would be influential spokespeople to meet with, who would be government persons that are steeped in the issue, so for example, in India, we know that some of the joint secretaries in the Ministry of Health and others like that are really working on tobacco control, so we work to set up those meetings, and also with our nonprofit partners, the nonprofit partners are receiving grants from us often, sometimes not, but frequently they are, and we set up meetings with those folks, individually and together, so we can hear their collective voice, and also their concerns, one by one.
I also find that it’s a moment when I can go to a restaurant and see, huh, is there smoking in this restaurant or isn’t there smoking in this restaurant? When I can look at some food in the grocery store and say, hmm, do these high-fat, high-sugar foods have warning labels or don’t they? Those kinds of things are very real when you’re on the ground, and it was opportunities like that that made the whole trip so valuable.
JAFFIN: Kelly, can you tell us about the countries that you visited, where did you go, what was this world tour?
DR. HENNING: We based this world tour on our focus countries, where we support tobacco control, so we have ten countries that are all low and middle income countries from all corners of the world that we support, to do best practice tobacco work. We also do other things in these countries, and often, we support things like obesity prevention or road safety work, but the backbone of the tour was to look at those ten focus countries, and so I visited Brazil and Vietnam, China and Indonesia, Philippines and Bangladesh, India, Pakistan, and Mexico, and you can see these are all quite large countries, so these are large, low and middle income countries with very big burdens of disease, and that’s how we decided where to go.
JAFFIN: And would you say that that’s the criteria for deciding where to work in general? Are there other specific criteria you look for when your team is choosing where to work?
DR. HENNING: So, we do look at burden. We look to see who has the largest number of smokers or the highest number of deaths from obesity and overweight, the highest number of road crash deaths, for example. We look at the burden very carefully, because we want to have the largest impact, and the way to have the largest impact is to put policies in place that affect the largest number of people. On the other hand, though, we do take other things into account, things like political will and interest in the problem, capacity of the government, and capacity of nonprofit partners. There are other things that we look at, but burden is really very important for us.
JAFFIN: And so given that you look also for good government partners, which is a theme in a lot of our work, something that we’ve seen in terms of our approach, working with cities, is that often, cities have similar problems that can be addressed similarly, and they tend to learn from each other. We look to facilitate that, but also, it happens a lot of times because cities near each other are facing similar problems. Do you think that government, national government, do they exchange ideas, do you think they can learn from each other, do you think this is a similar model with national governments?
DR. HENNING: I absolutely do. I think national governments really can learn from each other. They like to. They like to do things called study tours, where we put a group of officials together and bring them from one country to another, so they can see what’s going on, on the ground. Sometimes, that’s from a middle or low income country to a high income country, but sometimes it’s from a middle income country to another middle income country. It really depends on what’s happening locally. I also think that there’s a lot of competitiveness among national governments, so in tobacco control, the World Health Organization has the MPOWER Policies.
This is a package of things like smoke-free public places and pack warnings on cigarette packs and advertising bans. That package of interventions, the WHO grades those countries each and every other year, and when they grade those countries, countries look at those status reports and say, uh oh, we’re not really performing as well as our neighbor is performing on smoke-free, for example, so that does motivate lots of countries, so yes, I think this is a great model that Bloomberg Philanthropy uses overall, and it definitely works at national government level.
JAFFIN: We’d love to hear from you a couple of ah-ha moments, things that either surprised you on this trip, or that made you think about our work in a new way.
DR. HENNING: So, I’m going to make one comment about this that’s sort of large scale, and then I’ll kind of delve into a little bit of a smaller idea. One is that we work with ministries of health very often, and we provide lots of support to ministries of health. I mean, we’re the public health people after all, makes sense, but when I visit ministries of finance, who are so important to things like tobacco taxation, sugary beverage taxation, the ministries of finance say to me, please help us, the ministries of health need to be so much louder, so much more vocal to support our tax policies, and so there was kind of a disconnect happening in a number of countries between ministry of health work and ministry of finance needs, and so we can act as sort of the glue to try to bring those things together, and really try to advance things like tobacco taxation and sugary beverage tax that we know work and are really effective for public health, so that was a bit of an ah-ha for us, we weren’t expecting.
I think on a slightly more micro level, I was very surprised that this time, this past year of travel, for the first time, really, I started to see a lot of alternative products in tobacco, so things like e-cigarettes, heated tobacco products, a lot of concern by governments, a lot of concern by the public, and just a lot more in the marketplace than we had seen previously, and this is an area of concern, and one that we here at Bloomberg Philanthropies are taking really seriously.
JAFFIN: To that end, can you talk to us a little bit about what are some of the key ingredients that you’ve seen that can help a country tackle some of their toughest public health challenges? So obviously, having the finance minister tied to the health minister and echoing each other’s messages, breaking down silos, are there other key ingredients that you’ve seen?
DR. HENNING: So in the best of all circumstances, we have a really strong government with a lot of political will to work on public health policy issues, together with a really strong civil society group of organizations, because we really think we have to make sure governments have the capacity to act, and civil society is available to push governments to act in the interest of public health, so that’s really very important.
I would also say that we do see a lot of really interesting and important work in the legal area, so you may be aware that Brazil, just last week, filed a case on taking tobacco companies to task for having very high health costs to the country of Brazil, based on smokers and the illnesses smokers get, and so their government is going to now sue the tobacco companies to try to regain some of the health costs that they’ve incurred. This is a strategy that was used in the United States in the mid-1990s. It was used around that same time in Canada successfully, but really hasn’t been used broadly around the world, so Brazil is really going out there, trying to do some very innovative work, and so that’s another example of the kinds of things that can happen on the ground that really are impactful.
JAFFIN: So let’s stick with tobacco control for a moment, because it’s an area that we’ve been involved in for a very long time. Our founder and funder, Mike Bloomberg, took this on as one of the first things he did when he was mayor. We’ve been involved in tobacco controls, you noted, for 12 years, and we’ve put almost a billion dollars towards reducing tobacco use. So Brazil, great example, it sounds like that’s a real landmark case, and going to be a very big deal. Can you talk about other countries you’ve seen making real strides in fighting tobacco?
DR. HENNING: Yeah, we’ve seen a lot of progress over the last 12 years. It’s actually extremely exciting to talk about, and when we started back in 2007, about a billion people in the world had good best practice tobacco control laws in place. Now, we’ve quadrupled that number. There’s more than 4 billion people around the world protected by very good tobacco control policies. There are a couple of countries that are really moving forward quickly. Several years ago, Turkey became the first country in the world to have all of those MPOWER policies in place. Smoke-free public places, advertising ban, tobacco taxation, etc. Now, there are many countries that are starting to reach those levels and challenging Turkey. We even have progress in places where it’s very difficult. China, for example, is a difficult place.
The tobacco company is part of the government. It’s owned by the government of China, and yet, we have Shanghai and Beijing 100 percent smoke free. We have many other cities in China also moving ahead with smoke-free public places, and even Indonesia, which has actually been very far behind in terms of tobacco control, now has more than 100 cities who have become smoke free public place cities, as well as more than 20 that have banned tobacco advertising at city level, so we try to get national policy in place, we see lots of progress. If we can’t get that going, then we work at city level and try to get the cities to move the national governments, and one of my favorite examples is Bangladesh.
Bangladesh has lots of health issues. They have lots of infectious disease issues, they have many, many child health issues, but Bangladesh has actually managed to move so far forward that they’ve reduced tobacco use by 18.5 percent, and they have 3.5 million fewer tobacco users today than they did back in 2009, so I think many people wouldn’t imagine that Bangladesh would make that kind of progress, but we’re really excited to have been able to partner with Bangladesh on that kind of movement.
JAFFIN: So, even though we’ve seen a lot of success, we’re obviously committed to this issue of tobacco control for the long term, and even when we see countries like Turkey implement all of the MPOWER strategies, I know it’s constantly an uphill battle. Can you talk about some of the obstacles that countries face, even when they’re willing to do the most responsible things regarding tobacco control?
DR. HENNING: Absolutely. You know, the biggest obstacle that the governments and the nonprofits face are really the tobacco industry. The tobacco industry is extremely hard-hitting, they are very well-resourced, they do a lot of pro-tobacco advertising in these low and middle income countries, and they’re really moving outside of the United States in the high income areas, into the low and middle income countries, where there’s less capacity and less opportunity to be able to push back hard against the tobacco industry. They do a lot of things that we would never think about in the United States, things like major sponsorships of concerts for teenagers, or giving away free cigarettes on the street, or having their logos all over the jerseys of the soccer players on the field, things that, again, we don’t really see any more in the US or Canada or Western Europe, but that we are still seeing in a very big way in low and middle income countries, so fighting back against the tobacco industry is a major part of our strategy in the tobacco control work that we do around the world.
JAFFIN: And you and I have known each other for a long time and have worked together on public health issues, and specifically on the tobacco work for a long time, and so I remember, when we got started in this area, first of all, tobacco use was on the rise, and it has since leveled off and now started to decline globally, which you could say was unthinkable when we started. What other–what can other public health issues learn from the successes that we’ve had with tobacco, and are there lessons learned that we use that relate to some of the other areas we work in, whether that’s road safety or obesity or any other one you want to refer to?
DR. HENNING: So Allison, I think you know that–and the Public Health Team here at Bloomberg Philanthropies, we are really proud of the tobacco control work. We think it’s really central, but you probably also know that we build a lot of our programs on the strategies that we use in tobacco control, so for example, in road safety and in obesity prevention now, we have rapid response grants. These are grants that we can put out in the field very quickly, very low bureaucratic overhead, allowing catalytic change on policies in particular countries that really have an opportunity.
We also use a big, large, bold communication strategy, so we support partners in the countries in all of our program areas to make sure the public is aware of the dangers of these various products and situations, and to make sure that the message is really getting out there. That’s a major part, and I mentioned the legal strategies previously. It’s not so common to have philanthropic assistance around these legal pieces, and yet, countries are really clamoring for that sort of assistance, and so we find that that works across all of our initiatives, and we use it over and over and over again, so yes, tobacco is really our guiding star, we’ve used a lot of those strategies in many programs.
JAFFIN: So, it has been amazing to hear about the progress on tobacco specifically, and on other programs, and to see it firsthand, I think for you, probably going around the world, and obviously, none of this happens overnight, and it does take years, maybe decades, of strong leadership and committed partners, funders, and communities to implement these lifesaving policies. How can we now continue to support their efforts and spread the success to other cities and countries?
DR. HENNING: We have actually a new initiative called the Partnership for Healthy Cities that Mike Bloomberg began as part of his commitment to the World Health Organization role as the global ambassador for non-communicative diseases, and that partnership now has 54 cities as part of it and growing all the time, and the partnership cities are committing themselves to best practices around non-communicable diseases and injury prevention, and we’re really finding these cities are catalytic, and they’re really learning from each other, they’re learning lessons, and they’re disseminating the importance of working in these areas, so we really are excited about the idea that we have a groundswell of support for non-communicable disease work, and we’re hoping to continue to build on that as we move forward.
JAFFIN: So, if you had to sum it up, what makes you optimistic about the future of public health?
DR. HENNING: So, the world tour really made me optimistic, I have to say, and it’s definitely because of the people that I meet in each of the countries who are really passionate about this work, and who are so dedicated to pushing forward. They work in very difficult situations, they have a lot of industry pushback, a lot of long hours, late nights, and they never let up, so it’s very encouraging and very exciting to see that kind of commitment to public health, and I’m really happy to be part of it.
JAFFIN: Great, well, thank you for your time today and for the work you do all over the world.
DR. HENNING: Thanks, Alli.
OLIVER: We hope you enjoyed this episode of Follow the Data. Thanks to Kelly Henning for telling us more about her work.
If you haven’t already, be sure to subscribe to Follow the Data podcast. This episode was produced by Electra Colevas, Ivy Li and Jean Weinberg; music by Mark Piro. Special thanks to Eric Sheppard. I’m Katherine Oliver, thanks for listening.